Rectal Bleeding
Bright red blood mixed with or coating the stool. The most common presenting symptom of rectal cancer. Always requires investigation in adults over 40.
Call : 191 767 898
Most common GI cancer death
Precise local staging for all patients
Advanced sphincter-preserving surgery
Multidisciplinary team approach
Mr Kumar has advanced training in the management of rectal cancer, having completed specialist fellowships at two of Europe’s leading centres. He specialises in robotic TME, which offers superior precision in the confined space of the pelvis and is associated with better functional and oncological outcomes.
Mr Kumar offers the full range of modern treatments including organ preservation strategies and transanal approaches. He avoids a stoma wherever it is surgically safe to do so, and discusses all options frankly with each patient so they can make a fully informed decision about their care.
Confined to the rectal wall. Local excision (TAMIS) may be curative for very early lesions. Radical surgery (TME) for T2 disease and above.
Extending through the rectal wall or involving adjacent structures. Pre-operative chemoradiotherapy followed by surgery is the standard approach.
Bright red blood mixed with or coating the stool. The most common presenting symptom of rectal cancer. Always requires investigation in adults over 40.
Increased frequency, loose stools, urgency, or a feeling of incomplete evacuation (tenesmus), particularly new symptoms persisting for more than 3 weeks.
A persistent sensation that the bowel has not fully emptied after defaecation, a classic symptom of a rectal mass.
Unintentional weight loss is a red flag symptom that should always prompt urgent investigation.
Iron deficiency anaemia from chronic blood loss, presenting with tiredness, pallor and breathlessness.
Pain in the pelvis or perineum may indicate locally advanced disease involving surrounding structures.
Full colonoscopic assessment of the rectum and colon to identify the tumour, obtain biopsy for histological diagnosis, and exclude synchronous lesions.
High-resolution MRI is the gold standard for local staging of rectal cancer. It defines the relationship of the tumour to the mesorectal fascia (circumferential resection margin), guides surgical planning and identifies who needs pre-operative treatment.
Systemic staging to identify lymph node involvement and distant metastases.
All cases are discussed by the colorectal cancer multidisciplinary team, including surgeons, oncologists, radiologists and pathologists, before treatment commences.
After curative treatment for rectal cancer, close surveillance is maintained for at least 5 years. This includes:
Blood CEA measured every 3 to 6 months for 3 years as a marker of recurrence.
Annual CT chest, abdomen and pelvis for 3 to 5 years.
Flexible sigmoidoscopy or colonoscopy at regular intervals to assess the anastomosis and detect local recurrence or metachronous polyps.
Specialist assessment, MRI staging and robotic surgery under one roof.
Book a consultation with Mr. Lalit Kumar today.
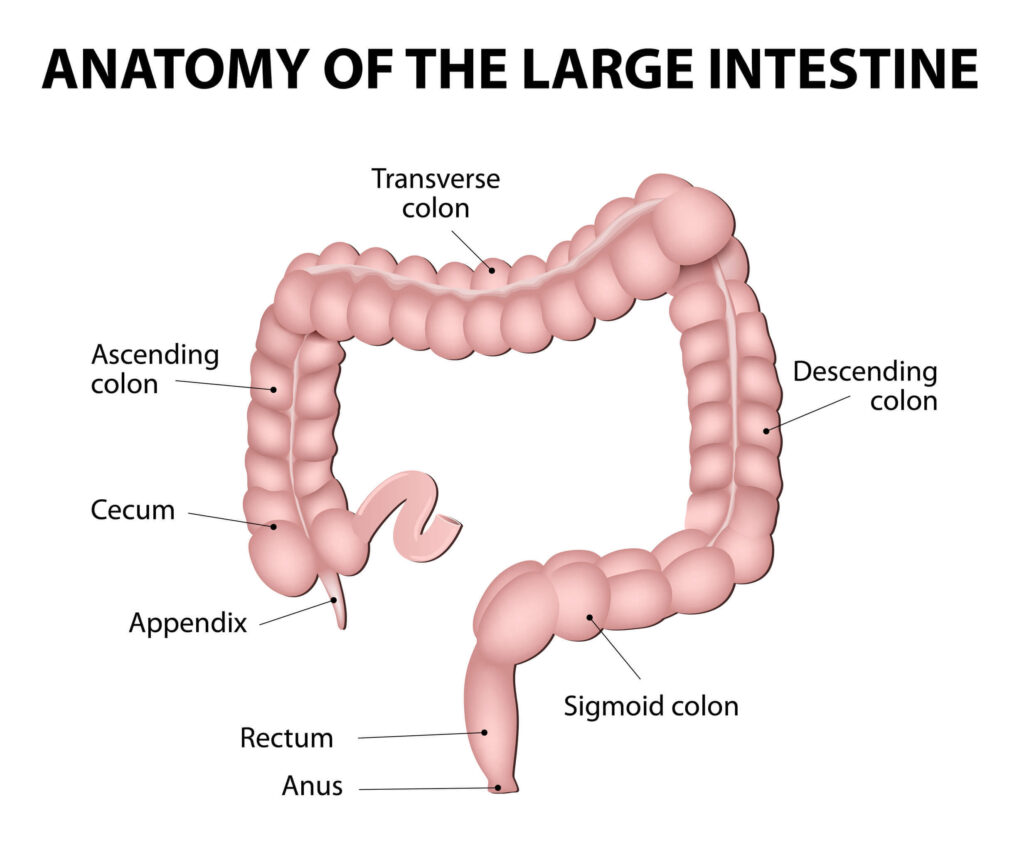
Anatomy
Large Intestine
UK incidence
TME local recurrence
Stage I survival
Robotic TME
Specialist opinion when it matters
Appointments typically within 3–5 working days.
Delivering high quality, patient-focused care
© 2025 West Midlands Surgical Centre. All rights reserved. · Privacy Policy · Terms & Conditions This website provides general information only and does not constitute medical advice. Always consult a qualified clinician.