Painless Bleeding
Bright red blood on toilet tissue or in the bowl, typically after passing a stool.
Call : 191 767 898
Adults affected
Resolve with lifestyle changes alone
Day case, no hospital stay, home same day
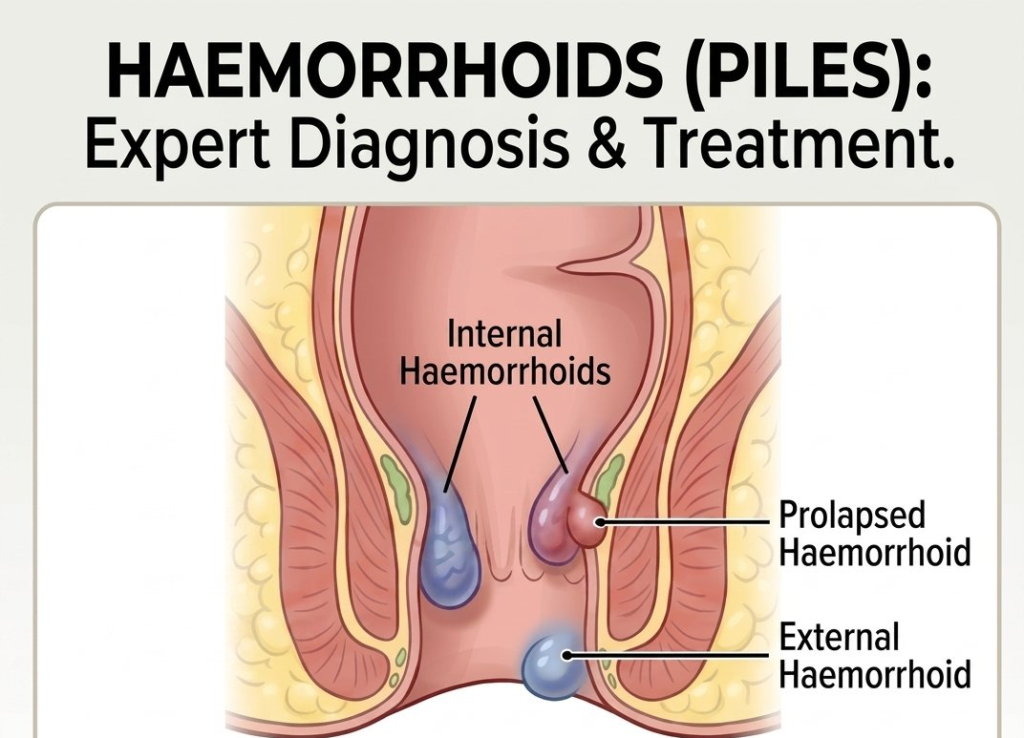
They can develop inside the rectum (internal haemorrhoids) or under the skin around the anus (external haemorrhoids). Both types are extremely common, affecting around 1 in 3 adults at some point in their life.
Located inside the rectum. Usually painless but can cause bright red bleeding and may prolapse during a bowel movement. Graded I–IV based on severity.
Located under the skin around the anus. Can be painful, especially if a blood clot forms (thrombosed haemorrhoid), causing sudden pain and a firm lump.
Symptoms can develop gradually and vary depending on the size and location of the haemorrhoid. Common presentations include:
Bright red blood on toilet tissue or in the bowl, typically after passing a stool.
A lump that pushes out of the anus during a bowel movement. May retract on its own or require manual reduction.
Persistent discomfort and itching in the anal region, often caused by mucus discharge from the haemorrhoid.
Typically associated with external haemorrhoids or a thrombosed (clotted) pile. Internal haemorrhoids are usually painless.
During your initial consultation, I will carry out a thorough assessment to determine the nature and severity of your haemorrhoids and ensure there is no other underlying pathology. This is a key reason why specialist evaluation is so important.
A gentle external inspection of the anal region to identify skin tags, external haemorrhoids and any other relevant findings. Performed with care and discretion at every step.
A brief in-office examination using a small, well-lubricated scope to view the internal anal canal. This is usually performed during your first visit and allows direct visualisation of internal haemorrhoids.
If there are red flag symptoms, or depending on your age and medical history, I may recommend a Flexible Sigmoidoscopy or Colonoscopy. These provide a complete view of the bowel and are arranged as a separate, scheduled procedure. This step ensures nothing is missed.
My approach to treatment is stepwise, beginning with the least invasive, evidence-based options and escalating only where necessary. The right treatment depends on the grade and type of your haemorrhoids.
Improving bowel habits is the most important first step. Many patients experience significant and lasting relief through these measures alone.
If symptoms persist despite lifestyle changes, internal haemorrhoids can often be treated effectively without the need for general anaesthesia.
For larger, more symptomatic, or persistent haemorrhoids, I offer several specialist surgical procedures performed under anaesthetic as a day case.
Self-diagnosing haemorrhoids can lead to delayed treatment for other, more serious conditions. Rectal bleeding in particular should always be properly investigated by a specialist. I provide a comprehensive evaluation to ensure your treatment is safe, accurate, and tailored to you.
Proper examination to exclude other causes of bleeding and rectal symptoms, including bowel cancer screening where appropriate.
A management plan specific to your grade of haemorrhoid, symptoms and lifestyle, not a one-size-fits-all approach.
Most patients are seen within days. Clinic-based procedures can often be performed at the same appointment.
Expert management can resolve most symptoms of piles effectively.
Take the first step, book a consultation with Mr. Lalit Kumar today.
Haemorrhoidal anatomy
Adults affected
Resolve conservatively
Banding success rate
HALO / surgical cure
Specialist opinion when it matters
Appointments typically within 3–5 working days.
Delivering high quality, patient-focused care
© 2025 West Midlands Surgical Centre. All rights reserved. · Privacy Policy · Terms & Conditions This website provides general information only and does not constitute medical advice. Always consult a qualified clinician.