Left-sided Abdominal Pain
The most common symptom of diverticulitis. Pain is typically in the lower left abdomen (the sigmoid colon), often constant and worsened by movement.
Call : 191 767 898
Over-50s have diverticulosis
Resolve with conservative management
Surgery when needed is minimally invasive
Diverticular disease is strongly associated with a low-fibre diet and is one of the most common conditions affecting the large bowel in Western populations. Most episodes of diverticulitis settle with conservative management, but recurrent or complicated disease may require surgical treatment.
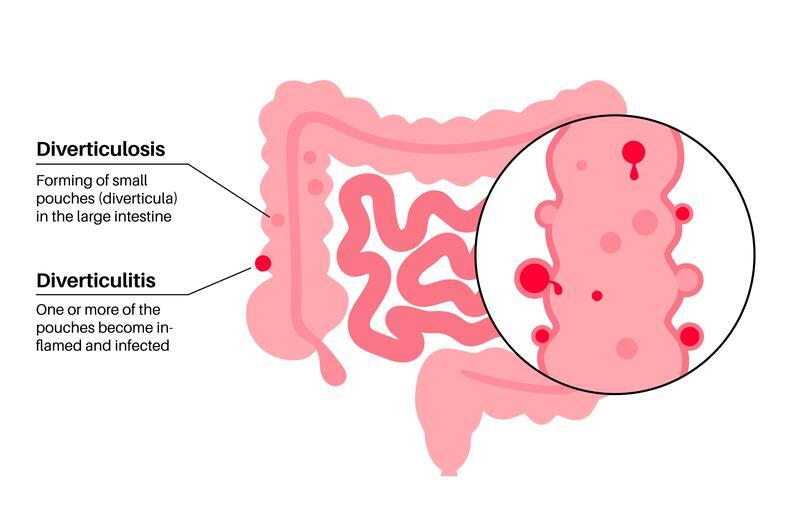
Diverticula are present but cause no symptoms or only mild bloating and discomfort. Managed with dietary optimisation. No surgery required in the majority of cases.
Inflammation or infection of diverticula causing abdominal pain, fever and change in bowel habit. Complications include abscess, perforation, fistula and stricture.
The most common symptom of diverticulitis. Pain is typically in the lower left abdomen (the sigmoid colon), often constant and worsened by movement.
Systemic symptoms of infection, including high temperature, chills and fatigue, indicate active inflammation or abscess formation.
Constipation, diarrhoea or alternating bowel habit. Rectal bleeding may occur from diverticular bleeding — which can be brisk.
Chronic diverticulosis commonly causes abdominal bloating, wind and generalised lower abdominal discomfort.
Diverticular bleeding can cause painless, heavy, bright red rectal bleeding. This usually settles spontaneously but requires urgent assessment.
Frequency, urgency or passing air or faeculent material in the urine (pneumaturia) suggests a colovesical fistula — a complication requiring surgical treatment.
History and examination to assess severity and likelihood of complications. Blood tests including full blood count and CRP.
The gold standard investigation for acute diverticulitis. Confirms the diagnosis, assesses severity, and identifies complications such as abscess, perforation or fistula.
Performed 6 to 8 weeks after resolution of acute diverticulitis to confirm the diagnosis, exclude colitis and ensure there is no underlying malignancy.
Diverticular disease ranges from a simple dietary condition to a complex surgical problem. Specialist assessment ensures accurate diagnosis, appropriate imaging, and a clear management plan — whether that is conservative, endoscopic, or surgical.
CT imaging and colonoscopy to confirm the diagnosis and exclude malignancy, which can mimic diverticular disease.
Conservative first, surgery only when genuinely necessary — tailored to your history and severity.
Laparoscopic and robotic colectomy for the lowest complication rates and fastest recovery when surgery is required.
Expert management can prevent recurrence and treat complications effectively.
Book a consultation with Mr. Kumar today.
Diverticular Disease Anatomy
Population affected
Uncomplicated resolution
Recurrence rate
Surgery needed
Specialist opinion when it matters
Appointments typically within 3–5 working days.
Delivering high quality, patient-focused care
© 2025 West Midlands Surgical Centre. All rights reserved. · Privacy Policy · Terms & Conditions This website provides general information only and does not constitute medical advice. Always consult a qualified clinician.