Intense Sharp Pain
Described as passing glass, the pain occurs during a bowel movement and may persist for minutes to hours afterwards.
Call : 191 767 898
Affects all ages and both sexes
Surgical cure rate
Day case, no hospital stay required
Fissures are often mistaken for haemorrhoids. The key difference is that fissures typically cause intense pain during and after a bowel movement, whereas internal haemorrhoids are usually painless. Getting an accurate diagnosis early is important, as an untreated acute fissure can become a chronic one, which is significantly harder to treat.
Present for less than 6 weeks. Fresh tear with sharp edges. Responds well to conservative treatment. Most acute fissures heal completely with the right management.
Persisting beyond 6 to 8 weeks. Often develops a sentinel skin tag at the lower edge. More likely to require medical or surgical intervention to achieve full healing.
Fissures produce a distinctive pattern of symptoms that usually allow a confident clinical diagnosis. Common presentations include:
Described as passing glass, the pain occurs during a bowel movement and may persist for minutes to hours afterwards.
Small amounts of fresh blood on toilet tissue or on the surface of the stool. Never altered or dark blood.
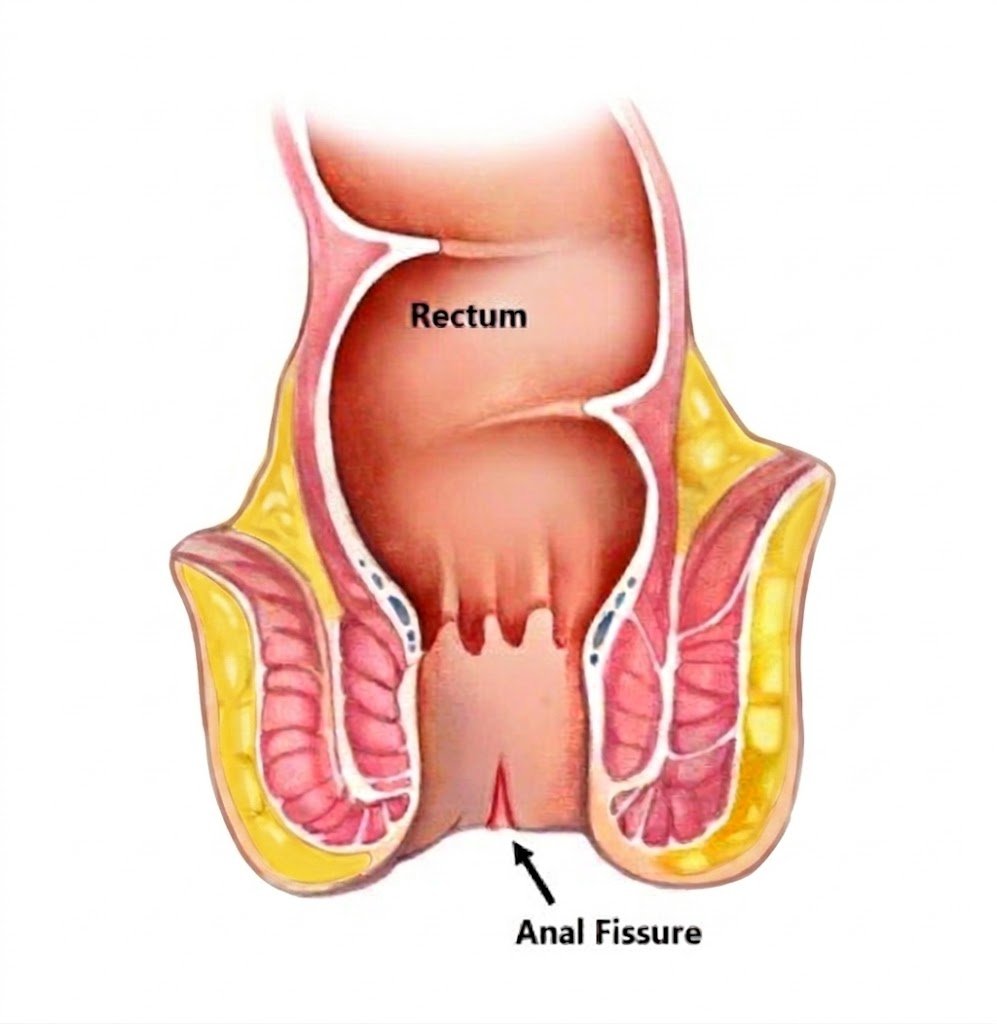
A small crack visible at the anal margin, or a skin tag (sentinel pile) that develops at the lower end of a chronic fissure.
Anticipatory pain leads patients to delay defaecation, which worsens constipation and prolongs the fissure cycle.
Anal fissures result from trauma to the anal canal mucosa, combined with reduced blood supply to the posterior midline, which impairs healing. Common causes include:
Straining and passage of large, firm stools is the most common cause. The mechanical shearing force tears the delicate anal lining.
Repeated passage of loose stool is an underrecognised cause, particularly in patients with inflammatory bowel disease.
Anterior fissures are more common in women and are strongly associated with vaginal delivery and obstetric trauma.
Crohn's disease and inflammatory bowel disease (IBD) can predispose to atypical, multiple or lateral fissures that are more difficult to treat.
Early intervention is key to preventing an acute fissure from becoming chronic. I use a gentle approach to assessment, ensuring your comfort at every step.
Most fissures are diagnosed by a careful visual inspection of the anal margin. Gently parting the skin is usually sufficient to identify the tear, a sentinel pile or any associated skin changes. An internal examination is deferred if too painful at the first visit.
To ensure the fissure is not a symptom of a deeper issue, such as polyps, IBD or malignancy, I may recommend a Flexible Sigmoidoscopy or Colonoscopy. These are arranged as a separate, scheduled procedure to fully evaluate the bowel.
I follow a step-up approach to treatment, beginning with the least invasive options and reserving surgery only for complex or refractory cases.
The majority of acute fissures respond well to conservative management. The goal is to relax the sphincter, improve blood flow to the area, and prevent further trauma from hard stools.
For fissures that have failed to heal after 6 to 8 weeks of topical treatment, a Botox injection into the internal anal sphincter is a highly effective, well-tolerated option.
Lateral internal sphincterotomy is the most effective treatment for chronic fissures, with healing rates exceeding 95%. It is reserved for cases where non-surgical and Botox treatments have not achieved healing.
A fissure that is incorrectly managed or left untreated can become a chronic, debilitating condition. Specialist assessment ensures the correct diagnosis, rules out underlying pathology and delivers a treatment plan tailored to your individual circumstances.
Proper examination to exclude other causes of bleeding and rectal symptoms, including bowel cancer screening where appropriate.
A management plan specific to your grade of haemorrhoid, symptoms and lifestyle, not a one-size-fits-all approach.
Most patients are seen within days. Clinic-based procedures can often be performed at the same appointment.
Expert management can resolve most anal fissures without surgery.
Book a consultation with Mr. Lalit Kumar today.
Anal Fissure Anatomy
Acute fissure healing
Botox success rate
Surgical cure rate
Recovery after surgery
Specialist opinion when it matters
Appointments typically within 3–5 working days.
Delivering high quality, patient-focused care
© 2025 West Midlands Surgical Centre. All rights reserved. · Privacy Policy · Terms & Conditions This website provides general information only and does not constitute medical advice. Always consult a qualified clinician.