Change in Bowel Habit
Persistent diarrhoea, constipation, or a change in stool consistency lasting more than three weeks, particularly in the absence of an obvious cause.
Call : 191 767 898
Most common UK cancer
Stage I 5-year survival
Minimally invasive surgery
Multidisciplinary team approach
The majority of colon cancers develop from pre-cancerous polyps (adenomas) over a period of years, which is why colonoscopic surveillance and the NHS Bowel Cancer Screening Programme are so important. Identifying and removing polyps before they become cancerous prevents bowel cancer from developing at all.
Confined to the bowel wall or nearby lymph nodes. Surgery is the primary treatment and outcomes are excellent, over 90% 5-year survival for Stage I disease.
Disease extending beyond the colon or involving distant organs (liver, lung). A multidisciplinary approach combining surgery, chemotherapy and targeted therapy offers the best outcomes.
Persistent diarrhoea, constipation, or a change in stool consistency lasting more than three weeks, particularly in the absence of an obvious cause.
Blood mixed with stool or fresh rectal bleeding without an obvious benign cause warrants urgent investigation to exclude malignancy.
Persistent or cramping lower abdominal pain, sometimes associated with bloating. Colic from bowel obstruction is a more urgent presentation.
Unintentional weight loss of more than 5% body weight over weeks to months is a red flag symptom requiring urgent assessment.
Iron deficiency anaemia caused by occult (hidden) blood loss from a right-sided tumour, often presenting with fatigue before any obvious rectal bleeding.
Inability to open bowels, vomiting and abdominal distension may indicate advanced disease causing obstruction, a surgical emergency.
The definitive diagnostic investigation. The entire colon is examined and any suspicious lesion is biopsied to confirm the histological diagnosis.
Staging CT to assess local extent of the tumour and identify any spread to lymph nodes, liver, lungs or other organs.
MRI for local staging of complex tumours; PET-CT to characterise indeterminate lesions or assess response to pre-operative chemotherapy.
All cases are discussed at the colorectal cancer MDT meeting, including oncology, radiology and pathology, to agree the optimal treatment plan.
After curative surgery, regular follow-up is essential to detect recurrence early. Mr Kumar provides structured post-operative surveillance including:
Carcinoembryonic antigen (CEA) is monitored every 3 to 6 months for 3 years as a marker of recurrence.
Annual CT chest, abdomen and pelvis for 3 to 5 years to detect liver, lung or other metastases.
Colonoscopy at 1 year post-surgery, then every 3 to 5 years to detect metachronous polyps or tumours.
If you have symptoms that concern you, specialist assessment is essential.
Book a consultation with Mr. Lalit Kumar today.
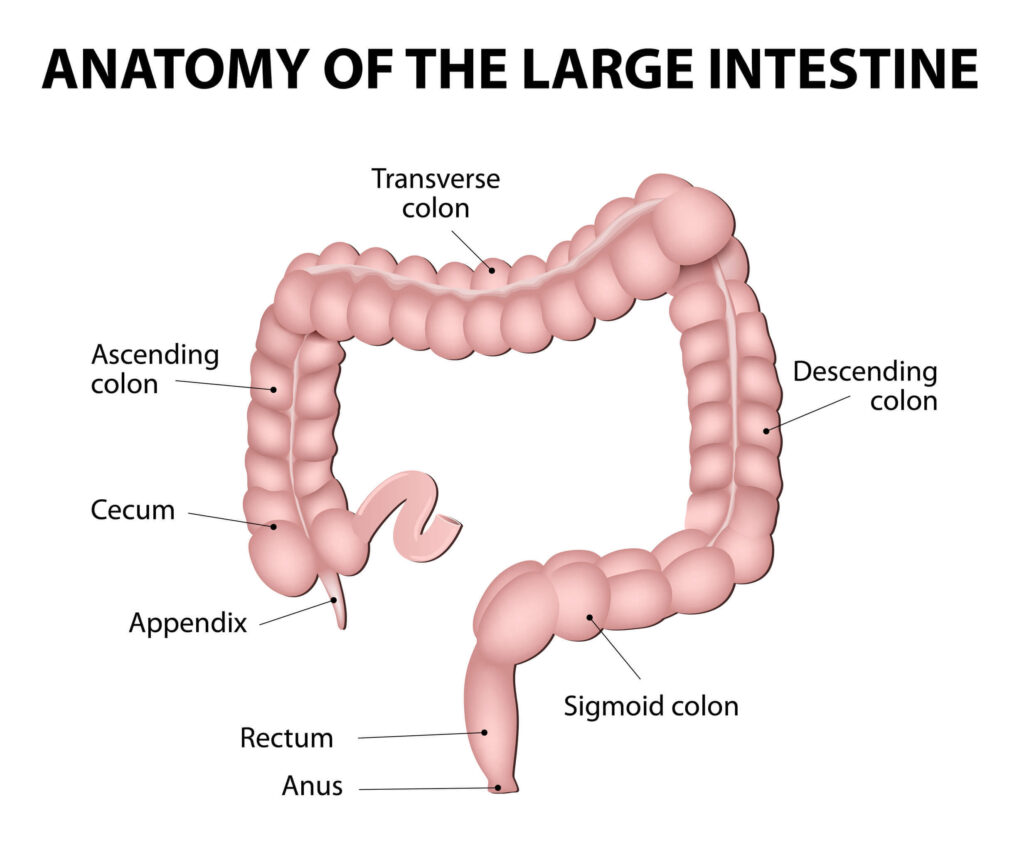
Anatomy
Large Intestine
UK incidence
Stage I survival
Stage III survival
Laparoscopic rate
Specialist opinion when it matters
Appointments typically within 3–5 working days.
Delivering high quality, patient-focused care
© 2025 West Midlands Surgical Centre. All rights reserved. · Privacy Policy · Terms & Conditions This website provides general information only and does not constitute medical advice. Always consult a qualified clinician.